Idioma:
Español
Fecha:
Subida:
2022-09-16T00:00:00+02:00
Duración:
1h 40m 43s
Lugar:
Espinardo - Centro Social Universitario
- Salón de Actos
Lugar:
Mesa redonda
Visitas:
1.377 visitas
Mesa redonda “Retos en investigación biosanitaria. Tendencias en salud y necesidades actuales"
CIBJI 2022
Descripción
Jornadas científicas
Transcripción
II INTERNATIONAL CONGRESS ON BIOSANITARY RESEARCH
FOR YOUNG RESEARCHERS
Welcome to this panel named "Challenges in biosanitary research.
Trends in health and current needs".
It is an honor to be here.
Thanks to the deputy dean for inviting me to this panel.
Since it's full of top-notch researchers
in different disciplines
from all over the world. Such as myself, since right now, I am in New York.
We're going to start with some brief presentations
and then we'll move on to a discussion.
Now, I'm going to introduce the speakers:
PhD Cyril Usi.
Researcher in the nanomedicine lab
in the University of Manchester, in England
PhD Ignacio Pedrinaci Pe~nalver.
Post-PhD researcher in Harvard 's School of Dentistry,
in Cambridge, in the United States
PhD Ana"is Jim'enez Reinoso.
Post-PhD researcher in the cancer immunotherapy unit of the research foundation of the 12 de Octubre hospital in Madrid.
PhD Miguel Gancedo.
A pharmacist and researcher in Astrazeneca,
in Cambridge, in the United Kingdom
And PhD Manuel Trinidad Fern'andez.
PhD in physiotherapy of the research group
of climetrics of the University of M'alaga.
Before beginning, let me introduce Pablo Pelegrin,
who is known not only in Murcia, but also outside of it.
He is the deputy director of IMIF, and the main researcher
in the immunology group of the biochemistry, molecular biology and immunology department of the Medical School of the University of Murcia.
Without further ado, PhD Cyril Usi has the word
researcher in the nanomedicine lab
in the University of Manchester, in England.
Thanks, Trinidad.
And thanks to the deputy dean
for inviting us to share our research in this convention.
I'm going to be the substitute of Cyril,
who couldn't be here today due to some last-minute problems
But we both work on the project I'm going to talk about.
I hope I can give young researchers an overview
of the biosanitary research we are currently carrying out
in the Murcian Institute of biosanitary research,
and in the University of Murcia.
Associated with other universities
and research centers at international level.
Our research project is funded by the EU programme Horizon 2020.
And our main objective is to design innovative tools
to study the impact and mode
of action of micro and nanoplastics on human health.
All of this, in order to create
a knowledge base for risk assessment
Our contribution to this project is focused
on the impact these micro and nanoplastics have on the immune system.
As you can see
plastics have been a major breakthrough for developed societies.
And, in fact, part of the industrial
evelopment of all Western countries
has been the use of these materials
because of their strength and flexibility.
However, many of these plastics are used only once
they pass into the environment very quickly,
and they do not biodegrade there.
So what happens is that, increasingly,
they break down until they generate very small particles.
these particles can reach
the micrometer or even nanometer scale.
The EU warned
that these plastic residues were being detected
in many ecosystems and were entering the food chain.
Therefore, the EU launched a call
to different research groups across Europe
to investigate the impact
of these micro and nano plastics on human health.
The whole environmental build-up is
to understand if there is really a risk or not.
For example, nanoplastics,
besides having a direct impact on human health
can be what we call carriers
of other pollutants, such as heavy metals
or even other types of pollutants such as bisphenol.
In this way, we would help
these toxins to enter the organism as well.
In this project there are involved
seven countries and 11 research centers from all over Europe
It is coordinated by the Autonomous University of Barcelona
so it is a project with clear Spanish leadership.
In Spain we also have the Institute of Plastics,
which is in Valencia and our research institute within this consortium.
In France we have two partners. In the United Kingdom
we have Dr. Cyril Busi at the University of Manchester
who was going to give this presentation.
We have a team in the Netherlands.
In Germany we have two teams.
And we also have collaborators in Denmark and Finland.
In addition to our project
the EU funded five other research projects
in the framework of the impact
of micro and nano plastics on human health.
Since they all have the same ultimate goal
the EU decided to make a research cluster
where we could all go hand in hand
and do research, not in parallel, but complementary to each other.
This large European research cluster
seeks to understand the impacts of micro and nanoplastics
and includes 71 institutions from 25 different countries.
It encompasses these five major projects
of which we, PLASTICHEAL, are part.
The other projects
are AURORA, IMPTOX, POLYRISK and PLASTICSFATE
which also include within themselves
other institutions at the European level.
What are we going to try
to investigate and what is our approach?
The project started very recently, at the end of last year
and we have funding until 2025.
So we are still at the beginning of this project.
The first thing we need to understand
is the environmental biomonitoring of these residues.
Where are these residues present?
They can be present in food,
in beverages, or in water.
And they can also be present in the air.
So the two preferred routes
of internalization of these micro- and nano-plastics a
re going to be the respiratory route and ingestion.
We are then going to study
the effects of these particles on the immune system
We are also going to study
their effects at the DNA level.
As well as their effects
on both the respiratory barrier and the intestinal barrier.
Their effects on secondary organs, such as the liver.
And their long-term effects
and the bioaccumulation of these residues in the organism.
We going to study this with different models:
From in vitro models to ex vivo models
using samples from patients
and people with exposure to these residues.
And in vivo models and
in silico models that will integrate all the data
Within the in vivo models
we are going to study organisms ranging
from invertebrates, such as the drosophila megalanogaster
to mammals, such as rodents.
We are also going to carry out a human biomonitoring
in which we are going to identify
the presence of these residues in populations
and identify high-risk populations.
All this, to carry out a risk assessment
and influence the regulations
governing the exposure of these micro
and nano plastics at European level.
This is a clear example of how
we are going to move
the most basic bio-health research that we find
into the new EU regulation several years from now.
This slide simply describes
the different work groups that we have
Work group number 1
is going to carry out an environmental monitoring.
Work group number 2
is going to perform monitoring in people.
Work group 3 is going to study the impact
of these residues on gastrointestinal and respiratory barriers.
Work group 4, where these residues go
and where they accumulate in the body.
Work group 5, the impact
on the immune system.
And work group 6, their short- and long-term effects.
And their effects on secondary organs.
All of this will go hand in hand and
will be synchronized with the risk assessment
and will influence the regulations governing the exposure
of these micro and nano plastics in human populations.
We lead our work group, which studies
the impact on the immune system
from the University of Murcia
and the Instituto Murciano de Investigaci'on Biosanitaria
In addition, we have the participation of
the Foundation for Health Training and Research of the Region of Murcia
the Regional Ministry of Health
of the Region of Murcia and the Murcia's Health Service.
Since we are going to have access
to patients who are being treated in hospital centers.
This is the whole team within our unit that is working on this project.
The Autonomous University of Barcelona and the Institute of Biosanitary Research Germ'an Trias I Pujol are also involved.
Both of them are associated.
We also have a French in our work program.
What are we going
to study within our work group?
Well, we are studying how
these plastic residues can induce genotoxicity in immune cells.
How they can change DNA
and oxidative stress in these immune cells
And how they influence the activation
and intracellular signaling of these immune cells
using proteomic and genomic techniques.
As well as their impact on oxidative stress on cell death, on the cell cycle and on the maturation and differentiation of immune cells
their impact on the activation of the inflammasome
since this is a field in which we are studying that it is a very important route for the induction of the inflammatory response.
And the effects of these particles on the activation of the immune system, but now in highly susceptible populations.
Finally, I wanted to show you some of the experiments
or some of the results that we have so far.
Here we have the incubation of macrophages,
which are highly FAO immune cells.
These have been incubated with polystyrene nanoplastics of diferent sizes that go from 100 nanometers down to 10 microns.
With them, we can study
how these particles are internalized in these cells
We can see how these particles accumulate in red in the cytosol of the cells.
In addition, with these cells we are going
to study how all the transcriptomics changes
how the internalization
of these particles regulates gene expression
and how the protein pattern
of these cells changes.
In addition, we can also study the release
of certain inflammatory mediators, such as inflammatory cytokines.
And here you can see how
by increasing the concentration of 50 nanometer nanoplastics
in this case polystyrene particles
it induces the release of the cytokine interleukin 1 beta.
This is a highly inflammatory cytokine.
On the right, you can see
how using macrophages of different genotypes
macrophages that are genetically engineered
to lose the expression of certain genes
these effects disappear.
Therefore, we can study which pathways are activating the exposure of these micro and nano plastics to induce the release of these inflammatory cytokines.
That'd be all! Thank you very much for your attention
and I will be happy to answer some questions.
Well Pablo, thank you so much for your intervention.
There is a guy who gave a lecture this morning
and told us a part of your work, which is very interesting.
So, we already knew something
And your partner in Manchester, Cyril, right?
He's running the nanoparticle part.
Well, first of all, any questions in the room?
Any questions?
Well, you are already a senior.
You have just jumped the step from junior to senior.
I wanted you to tell our young researchers a little bit
about how you come to conceive a European project of this size
and to collaborate with so many partners to achieve a common result.
How difficult is it or what are the challenges you have faced
and the advantages of being able to work like this?
Yes, it is complicated.
It is complicated because the European Union is highly restrictive.
And it is very difficult to get European funding.
One of the main aspects that I think
is essential for research at all levels is:
the more ideas you have and the more projects
you propose, the more chances of success you have.
For example, this project, which is very exciting for all of us
has cost us a lot of money. It has not been the first time
we have presented ourselves for a European project.
So, maybe out of ten projects that are presented, we get funded for one.
You have to be very persevering
and try to apply for funding through various channels.
In the case of European projects, you need
to have a network of collaborators and contacts at national and international level.
It is very important that you create these networks
from the very beginning of your research career.
It is essential that you find your niche in research.
Because when you have a niche and you can grow within it, you start to be known internationally and that leads you to generate this network of collaborators.
Therefore, once these calls from the European Union appear
you have to see if they could partner with you
to be able to ask for this project at international level.
I did my postdoc near Manchester, but I have never seen Ciryl's group before.
These are very big universities, where there are many groups
and each one is studying their independent projects.
And it is very nice and interesting to be able to collaborate with all these groups
especially with international networking.
Did you hear that?
Okay. Trinidad, I don't know if you can hear us, if you can intervene.
Well, another question addressed to the young people
who have little intention of participating. They are a bit shy.
How important do you think it is that, before finishing their degree,
they know how to speak English and how to express themselves correctly?
How important it is that they leave their country and get to know other realities?
How important do you think it is for the integral formation of a researcher that they carry out this series of activities?
Because you have been working in Manchester.
Maybe that has given you experience, knowing how to work in a different way, and contacts that become a possible future networking.
Indeed!
I did my PhD at the University of Murcia.
I am very happy to have done my predoctoral training.
Because in Spain, we know how to train people very well.
People are trained hand in hand with researchers,
university professors and researchers at research centers.
But once you are trained, you have
to go out and get to know and make yourself known.
I realized the importance of this networking once I was abroad.
And I was very lucky because at that time
Any researcher who came
to the University of Sheffield, where I spent 3 years
and to the University of Manchester, where I spent another 3 years
would rotate with all the researchers in the lab.
Then we would sit with them and personally tell them about our project.
And we had direct feedback
from those researchers and we got to know them very closely.
That's when I realized
how important it was to have this network of contacts
Can it be done from Spain?
Probably, but it is more difficult.
In Spain there are less researchers coming
to the research centers, or the departments where we do our PhD.
It is very important that once we have
our initial training as doctors or as bachelors, as masters
we go to other universities and other research centers abroad.
It is not essential, but it is advisable.
In Spain we have very prestigious centers.
In Madrid you will all know Zenit and Genio,
which are structures of the Instituto de Salud Carlos III
to study oncological and cardiovascular diseases.
These centers also attract a lot of foreign researchers.
And there is a lot of exchange of ideas and knowledge.
So, in Spain it is also possible to make these types of contacts.
But abroad, you are going to improve your English.
You are going to improve your understanding
and you are going to face another lifestyle.
And that also awakens many parts of the brain that are normally asleep.
And you stop thinking that things
are the way they are and assuming them as they are.
Going abroad is very good for many aspects,
but for the scientific career I think it is necessary and essential.
Thank you very much for your intervention.
Now we are going to give way to the next speaker.
I hope we will have time for all of us and the participants
to have a little debate on what is hot right now in research.
Thank you very much, Pablo Pelegr'in.
We give way to Dr. Ignacio Pedrinaci Pe~nalver
who is right now at Harvard, in Cambridge,
in the United States, with its time difference.
Welcome, the floor is yours.
Hello everyone, can you hear me?
Yes.
Well, right now I'm at the airport
so I had to stop at a coffee shop.
I hope the noise isn't annoying.
I'm in a small room where there are no people.
I didn't want to miss this event
and I was really looking forward to it.
I wanted to thank you for counting on me.
I consider myself young, a young researcher.
When they contacted me
my idea was to share a little bit of my background
and to give some ideas for
other young researchers who wanted to make a career in research
n any of the branches of the health field.
I am a dentist.
And in dentistry, as in medicine,
as in nursing. or in any other degree
we have research opportunities
that during the degree, nobody tells you about.
And you think that by doing psychology
you are going to have to work in an office
or by doing dentistry, as in my case,
you only know how to do fillings or remove teeth.
And you couldn't be more wrong.
I had a slide that I'm going to try to share so I can show it to you...
If I can't, that's okay.
Can you see it?
It's just a timeline.
Anyway, I'm from Granada.
But, when you come from a small city
or maybe you don't come from a university as big as the UGR
it's normal to be afraid and undervalue yourself.
And you think that because you are from Madrid or from Boston,
you are not going to reach their level and you are going to be the worst.
And this was the first thing I wanted to address today.
And nothing like that, everyone has their worth, their appeal.
And it doesn't matter what university
you are in you can reach your full potential.
In my case, I went on Erasmus.
I did an Erasmus in Norway, I went to Oslo.
I spent there the fourth year of my degree.
It was the first international experience in which I could see
how differently a dental school worked from what we had here.
And I realized that the main difference were the means.
Maybe we had here the latest dental chair and the latest light
but the treatments were still the same.
And going abroad was a way
of exploring those options that weren't available in my university.
I thought that in Europe I was limited
and I decided to pursue the American dream, like in the movies.
I did three stays during three different summers.
Every summer, when we had holidays in Spain
which is something you don't always have in every country, I miss them now.
I went to the University of Michigan in Ann Arbor City.
I went to the University of Iowa, in Iowa City.
For my last stay, was able to go to Brazil, to the University of Sao Paulo.
So, I was able to see different concepts of their ideas thanks to scholarships.
Everything I have achieved throughout my professional research career
has been thanks to scholarships and grants
from the University, from the Spanish Government, or from companies.
These scholarships are available for everyone.
You just have to look them up on Internet or talk to as many people as you can
using that Networking you were talking about.
Start drafting your resume, your motivation letter...
Don't limit yourselves thinking this is not for you.
Don't think that you have nothing to offer
compared to others.
Even if you think that you are not as smart
or as good of a dentist
asking for scholarships gives you the opportunity
to visit other centers, other places and discover what you like.
It's wonderful to be able to travel, meet other people.
You get to talk to post PhD, and they tell you about their projects...
and that's the best way to know what you're interested in.
And all of this is easier than it seems.
Now, the last scholarship I got and that got me into Harvard University
was from an international private dental implant company.
And even with my resume, I thought I had no chance, but I applied for it.
With a good motivation letter, a good level of English and hard work, I got it!
That's why I'm doing my post PhD here.
I also started as a faculty in the department I joined.
As you can see, everything fall back into place eventually.
At the end of the day, I have lived in 3 continents and 6 countries
all by working hard. I'm lucky enough to love what I do.
I was asked to give some advice on
how to encourage young people to join research.
First, you can't go anywhere
without a good level of English. It's your way of communicating.
Luckily, young people have more interest and are more devoted to learning English
since elementary school. My nephew knows more than I do, for sure.
And you should really work on your English. It will be useful for everything you do.
Secondly, make contacts.
People can give you a lot of opportunities.
When they don't know who to call
for a project, they will count on someone they know.
Lastly, apply for all the scholarships and grants there are.
Even if you think you are not good enough, it's free to apply, so just do it!
That's all! I just wanted to share my experience.
And answer any questions that you guys may have.
Thanks, Ignacio.
Any questions?
A student has a question for you.
Alright!
Okay, so he's studying medicine at University of Murcia.
I don't think you'll hear him, so I will listen first and I'll relay the question to you.
First of all, good afternoon!
I wanted to ask what is it like to go to another university?
Because it's not the same to look for a job, or do research
in your own University,which you know how it works.
As it is going to another completely different place.
What is it like to go to an unknown University
and trying to make your way? Especially in a renowned University...
Did you hear him?
So,once you have studied at a university, in this case Ignacio studied at the University of Granada
how do you go to another university?
You have talked about scholarships, you have to look for them.
How has it been for you to go
to another place of which you know nothing about?
How do you come up with it? How do you find the information?
How did you say one day when you were in Granada: "I'm going"?
I've always been a bit restless and I've always wanted to travel.
So I applied for an Erasmus Plus.
A program organized by universities all through Europe
in which you can spend a year of your degree in any other part of Europe.
I think it should be mandatory.
It's wonderful. Not only because of the people you meet
but also because you can see how
your degree works in other universities.
You see that others aren't better, I have been very disappointed..
I also talked with professors at my university.
In summer, I did a fellowship of two weeks or ten days during summer in the United States.
I talked with professors at the University of Granada who did research
And just like the other speakers here today, they have contacts at a lot of universities.
Researchers are always going to be open to visits, to help
because it's a generous field.
I have never been turned down when I have sent an email
asking to visit a university, a dental clinic or whatever.
I also moved to Madrid to do a Research Master in Dental Sciences
at the Complutense University, I didn't know anybody there.
I once you have been doing research for a year, you get to know your professors, your classmates, the tutor of your end-of-degree thesis and you have contacts again.
This allows you to make other contacts and to visit another university...
That's my experience.
Did I answer your question?
Did he?
So, regarding the role of mentors...
So, as you said, it's important to be brave enough
to leave your comfort zone and your environment.
Spain's SICUE, Europe's ERASMUS, Latin America's ILA
and, sometimes, even USA
is a temporary exit. You go for
a while and you know that you'll come back.
It's just for a few months.
It's a very enriching experience.
In medicine we have a high mobility rate, as do the rest of the degrees.
My question is:
Do you think that teachers, professors, researchers have an important role
in mentoring to put students who have these concerns in contact with other groups?
For sure.
I was very lucky in my degree to find my mentors
that, throughout my career, have been constantly changing.
The one I currently have
keeps inviting me to give lectures that he cannot attend
or suggests that I do an article.
Mentors are going to help you
make your way. They are a bit like your parents.
If I were a student mentor, which I have not been so far
I would tell them a little bit about my background.
I would offer him to be at the University where I am.
Sometimes you are hard-working and everything
but you need a little push, or a little help...
So, look for a good mentor who has good contacts and who cares about you.
Thanks! Any more questions?
Our vice dean of dentistry has a question.
I'll tell it to you directly, Maria. First, I want you to thank him on my behalf.
We've learned a lot from his talk. We were
all very much in admiration and very envious too
And I wanted to ask him
if he thinks that the undergraduate curricula
in general, I think for dentistry and for other degrees
if we can improve the student's training in research and promote it too.
If they are encouraged to do research.
If there is room for improvement.
At his university?
In general.
Okay.
They express their gratitude and envy for your career and the example you set for young people.
What do you think about the curricula of dentistry and other biosanitary degrees?
Is there much room for improvement
of these curricula to properly train professionals in research?
It's frozen...
Something happened to PhD Trinidad Herrero that is very common when you are in healthcare centers, in hospitals...
there are firewalls, the Internet networks cut communications for protection.
She is in the United States so she has no data on her phone.
She cannot moderate because she cannot hear us from inside the hospital.
Ignacio is at a cafeteria next door, it could be that the connection was unstable...
Fortunately, we have heard a good part of his talk.
So, we will save that question for when he is back.
So, let's move on to the next speaker.
Hi Ana'is!
Ana'is Jim'enez Reinoso is a post-PhD researcher at the cancer immunotherapy unit
of the Fundaci'on de Investigaci'on 12 de Octubre in Madrid.
You were going to be here live and at the end it wasn't possible.
We can see and hear you!
Thank you very much for attending.
Tell us a little bit about your background, what you do.
I'll tell you a about it at the end if there are questions.
Can you see the presentation?
I don't know if you see it...
Can you see the presentation?
RIght now, there are a lot of things on screen...
Good afternoon and thanks for having me.
I'll talk about my background later.
First, I want to show you what we do in our research group.
We focus on T-lymphocyte redirection strategies for cancer immunotherapy.
Within the wide range of varieties of types of cancer monotherapy
as cancer vaccines, oncolytic viruses,
immunomodulators checkpoint inhibitors whcih might have heard of.
Targeted antibodies, both monoclonal and biospecific
medication and there is the so-called adoptive cell therapy
which is what I am going to dwell on.
They can be endogenous and use
cells that are within the body to combat tumor cells
or artificial.
So, the cells such as T-lymphocytes,
ANKs cells, recently also macrophages are modified
so they express receptors on their surface,
or secrete molecules to favor their anti-tumor efficacy.
I'm going to focus on the ones
we use the most in the laboratory: TILs or tumor infiltrating lymphocytes
when treating lung adenocarcinoma
in non-small cell lung carcinoma
and in the generation of STAb-T cells, compared to CAR-T therapy.
What are tumor infiltrating lymphocytes?
It's s a therapy that is used primarily for solid tumors
and consists of isolating cells from tumors that are extracted, activated outside the body.
their proliferation is favored and then they are fused back into the patient.
Once fused, these cells go back to the tumor through chemokine, through receptors
and release mediators that produce the lysis of the tumor cells.
TILs are mainly T-lymphocytes.
There are also, in some cases, ANIK cells.
Their use has been extended mostly for the treatment of metastatic melanoma.
There is no FDA-approved therapy as such today
but there are lots of clinical trials
that showed effective responses in metastatic melanoma.
As you can see, after 80 days
of treatment, this tumor has practically been eliminated.
The use of TILs therapy is not current
but there're many trials going on right now-
The Rosenberg Group was the first to use
these therapies that included the infusion
of these cells with high doses of IL-2 and especially in melanoma.
Here you can see two recent trials
in metastatic lung cancer that are quite promising.
In September, at the ESMO Congress
researchers showed the results
of the treatment of TILs against metastatic melanoma
in a phase III trial and how its efficacy is more
than double that obtained with a classic melanoma-approved treatment
such as ipilimumab, which is a checkpoint inhibitor, an anti CTLA 4.
These TILs have also been genetically modified to increase their cytotoxicity.
These TILs have also been genetically modified to increase their cytotoxicity.
They have a greater antitumor capacity
so they are more effective at finding tumor cells, which is called tumor homing.
And also to reduce their exhaustion
since once these cells are extracted
from the tumor, amplified ex vivo, and re-infused
it's likely that once
they begin to act, they are exhausted and their efficacy drops.
When it comes to artificial adoptive cell therapies
we find the T-cell redirection strategies, which we also work on.
These can be MHC-dependent
which is the modification of blood cells, of peripheral blood lymphocytes
so that they express a specific TCR with high affinity against tumor antigens.
But we need a series of cell clones that are of the same type of MHC so that they can act.
On the other hand, we have MHC-independent strategies.
such as chimeric antigen receptors,
for example CAR-Ts, which you have probably heard of
or bispecific antibodies, which have two specificities.
With CAR-T therapy
CAR-Ts are antigen receptors that
would be based on the structure of a TCR lymphocyte
a T-lymphocyte receptor whose components are modified.
So, basically they are formed by a combination of the receptor that recognizes the antigens
alongside other series of co-stimulatory molecule domains
to favor their activity, activation and persistence.
Since the first generation of these cases was generated
different models emerged.
These consisted of modifying these co-stimulatory domains
to favor their cytotoxic activity, to reduce their cytotoxicity at the systemic level
and to favor this proinflammatory environment, for example, by releasing cytokines.
Here is a list of the approved CAR-T therapies for hematological tumors
with which they have been
most successful, especially in type B malignancies
We have also tried to use this therapy in solid tumors
but accessibility in solid tumors is more complicated.
Plus, the tumor microenvironment is more complex
and immunosuppressive for the arrival of these cells.
Antigens against which these receptors are made
are not only expressed in tumor cells
but also in healthy cells
generating on-target and off-tumor toxicities.
they detect the antigen against which
they have been manufactured very effectively
but they are very toxic for healthy cells.
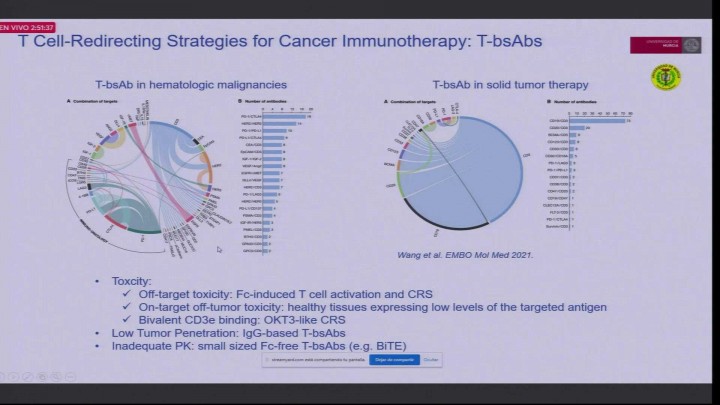
We also have the use of bispecific antibodies
which are injected in a soluble form and in different formats.
There are different types, some are larger, some smaller.
Being larger could favor the arrival
but produce other cytotoxicities associated with
the IG domains of the immunoglobulins from which they come.
Smaller ones can be eliminated more easily
but more reinfusions would be necessary.
There are also some clinically-approved.
One of them is blinatumomab for the treatment of refractory B neoplasms
an antibody that recognizes
the tumor-associated antigen CD-19, which is present in these B-type tumor cells
and binds to T-lymphocytes, which are responsible for mediating this crisis.
They have also been used for solid tumors
and, as CAR-Ts, they have
off-target and on-tumor toxicities
as low penetrance and low activation over time.
In our group we focus on a therapy called STAb
which stands for: secretion of T-cell redirecting by specific antibodies.
It consists of modifying mainly T cells
so that they secrete bispecific antibodies.
We have the advantages of CAR-T therapy
like activation of T lymphocytes,
which have been genetically modified to grow bispecific antibodies.
And the advantage of bispecific antibodies injected in a soluble form.
And, these cells that secrete bispecific antibodies are capable
of recruiting other cells that have not been modified but that will have cytotoxic activity.
If they were injected into an area of a solid tumor
they would favor the activation
of tumor infiltrating lymphocytes of the tumor.
And the systemic toxicity associated
with CAR-T therapy and bispecific antibodies would reduce.
I am going to give two more examples of two projects.
The first one, uses STAb and CD19 cells,
and we have already started a phase 1 clinical trial.
We focus on generating T lymphocytes,
which secrete a bispecific anti-CD3 and anti-CD19 antibody.
On the one hand, the T cells recognize this antibody and eliminate cells expressing CD19.
Compared to CAR-T cells, CD19 cells, the ones that are being used nowadays
are able to secrete this antibody detected by a Western Blot.
This antibody is able to bind to these own cells
in a phenomenon called decoration that we can visualize here by flow cytometry
The activation of these cells, which occurs through an immunological synapse
has a phenotype more similar to a canonical immunological synapse
compared to synapses mediated by CAR-T cells
which are less similar to what would occur physiologically.
We have proven their greater efficacy compared to CAR-T therapy with in vitro trials
both in real-time cytotoxicity trials
CAR-T or STAb-T cells are cultured in vitro with tumor cells
and over time, we visualize and quantify how these tumor cells are dying.
The efficacy to eliminate these cells is greater in STAb cells than in CAR-T cells.
This cytotoxicity is also favored because
the STAb cells not only eliminate tumor cells
but also through the recruitment of other cells
that have not been modified, but also have a cytotoxic behavior
all this increase in cytotoxicity is favored.
With in vivo trials, we have seen
that these cells are able to increase long-term disease-free survival.
If we compare the survival of mice that have been treated
with tumor cells and then with CAR-T or STAb-T cells
the survival of mice treated with cells
that secrete this bispecific antibody is of one hundred percent
whereas, at the beginning CAR-T cells are very efficient, but they lose that efficiency over time.
Same thing happens with the amount of cells expressing tumor cells over the days after this injection.
We have carried out a project very similar to this one,
focused on the treatment of T lymphoblastic leukemia
against the tumor-associated antigen CD1a.
These experiments are very similar
to the ones I've shown you and prove the same:
That STAb-T cells (CD1a) are more effective
even at times as short as two hours compared to CD1a-CART cells
at different effector and target ratios.
In trials in which we cultured non-transduced cells with transduced cells
the secretion of this bispecific antibody through a system called Transwell
is able to pass through this secreted antibody,
recruit the cells that are in this part of the Transwell, and favor tumor cell cytotoxicity.
We've also seen this with CD1a cells in vivo.
In this luminescence trial you can see
how the mice that have been treated with STAb, except for one
have remained disease-free over time.
So, we believe that STAb-T therapy is very promising
and we can add it to the compendium of therapies that exist for the treatment of cancer
both for hematological and solid tumors.
Thanks to everyone, to members of my research group, and others who have collaborated
with patients and with all sorts of trials.
Thanks! If you have any questions about my background or whatever, let me know.
Thank you, Ana"is, that was super interesting.
Your work perfectly frames the current challenges.
You studied at Universidad Aut'onoma de Madrid, right?
Well, I studied biology at Universidad Aut'onoma, then I went to Complutense
where Idid a master's in biochemistry and biomedicine.
I did my thesis on Immunology
and the complement system. I've studied the immunological pattern of T lymphocytes
Now, I'm bringing that together with cancer and immunotherapy.
Any questions?
I wanted to ask you about the limitations and advantages of immunotherapy for cancer, because it is a really powerful field for research.
which is opening up possibilities
of clinical treatment for patients and tumors that until now could not be reached.
But all this has a series of limitations, side effects, right?
There are a lot of limitations, mainly economic limitations.
These therapies are quite individualized.
Ideally, these therapies would be available for everyone, as other treatments are.
I am talking about STAb and CAR-T therapies.
For example, they are less toxic than CAR therapies
but they have some risks, such as cytokine vibration syndrome.
These toxicities have been causing problems over the years.
For example, the efficacy of TILs after reinfusion has not been as great in some cases as in others.
As you could see in a graph with
the preliminary data from that trial 3, in some cases it is very advanced.
They are very promising. Which reopens the discussion to go back to TILs.
Which are only being used in a hospital in Israel.
So, the advantages are: until now, they have been highly efficient
but they are not normally administered as a first option.
And many patients would benefit more
if they were administered these therapies at first, not when there is nothing else to do.
Or as a combination of therapies that are being given in parallel to favor earlier antitumor efficacy.
Thanks! Any more questions?
Well, let's move on, and see if we can have a discussion all together afterwards.
Thank you, Ana"is. Now Miguel Gancedo has the word.
Miguel is in Cambridge right now, if he has not gone on another trip, where are you?
Hi! Can you hear me?
Miguel Gancedo is a pharmacist trained at the University of Murcia
and now he wokrs at Astrazeneca.
Thank you very much for your time. The floor is yours!
Can you hear me?
Well, first of all, thank you for having me! I'm glad to see familiar faces here!
I studied at University of Murcia
I studied pharmacy and I'll tell you about my background later.
But today I want to talk about something
that is not so well known in the academic field:
how therapies or molecules are discovered and which are being used in clinics.
I'm going to share some slides. I hope you can see them.
Yes, we can!
These slides sum up what is done in the pharmaceutical industry
from the moment we identify a molecular target
that we want to treat by inhibiting it with some kind of pharmacological modality
until we get to the clinical and regulatory stages.
Most of you know Astrazeneca because of the coronavirus vaccine.
But today I'm going to talk about something different
that I hope will help students find options
that are not so well known, especially in the pharmaceutical, medical and biochemical fields.
Here I highlighted the different therapeutic areas in which Astrazeneca works for the R&D Department, in which I work.
I'm in Cambridge in the UK. This is the building that, hopefully, we'll be moving into next year.
It's located next to a health campus, which I'll refer to later on.
Astrazeneca focuses mainly in oncology, although we also work in other therapeutic areas
such as cardiovascular neuroscience, immuno-oncology, and now, rare diseases by the decision the company Alexia.
Recently, Astrazeneca announced its plan
to create an R&D headquarters in Barcelona focused on rare diseases.
In Astrazeneca there are currently 184 different projects
focused on trying to discover specific molecules or drug therapies
for different molecular targets,different indications, and different pathologies.
Right now, in Astrazeneca, there are about 76,000 employees.
It's a huge multinational company, but the main R&D headquarters are here.
Most of you are familiar with more traditional therapies,
such as small molecules, which are the most well-known therapies or monoclonal antibodies.
Ana"is has talked about bispecific antibodies
conjugated with different medication, even with cell therapy.
These different pharmacological modalities are being very actively investigated in the pharmaceutical industry.
There are other modalities, that are not so well known
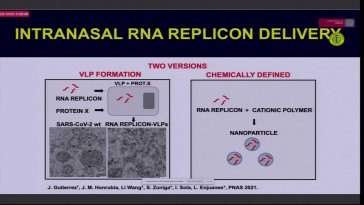
These will have quite an important impact in clinics in the next 10 years.
Like PROTACs, which is the second picture we have here.
Let's imagine a simple medication that has two pharmacophores
one will bind to the target molecule, and the other to an E3 lyase.
E3 lyases are enzymes that are in charge
of ubiquitinating proteins and degrade them in the proteasome.
They are degradation therapies for a specific protein.
There are other nucleotide-based therapies,
such as MRNA, which you will know from the COVID vaccine
or silencing RNA.
I think at the academic level, we know
very well he stages of discovering and developing new medication.
from the preclinical stage to the clinical and regulatory stage by the SDS, or the EMA.
But previous stages are not that well known.
Biochemical and molecular research makes it possible
to identify molecular targets that can have a direct effect on different pathologies
And to find chemical molecules and a way to optimize them
so that they have a specific, safe and pharmacological effect for a specific population segment.
The process from the identification of the molecular target, the protein that we want to inhibit or modulate
until it is commercially approved, takes around 10-15 years.
The most crucial part that must be taken
into account in order to one of these molecules to be successful
to be marketed and not to fail in the clinical stages, where drugs are most often withdrawn
is the first part, which is responsible
for determining the exact molecular target that we want to identify.
In this sense, biomedical research and clinical data are extremely important
to know which genome is associated with different diseases, such as different tumor cancers.
For this, many technologies are used at the industry level, such as gene editing screening,
using an enzyme called CRISPR/Cas9
that activates, inhibits or eliminates different genes from the genome.
This way, we know the phenotypic effect it has on different cell types.
Once the protein we want to target is identified and validated by in vitro trials
We know the biomarkers on which we could base
to know if the appropriate indication is being regulated as we want.
Once we confirm that this protein
can be studied, we start finding chemical molecules.
We screen billions of molecules.
This is where I am involved in, which is pure molecular biochemistry.
With several techniques we identify chemical molecules
that are going to bind in different parts of the protein through molecular interactions.
Then, we validate by different types of trials
if these molecules have an antagonist or modulatory pharmacological effect.
A very innovative technology that I am quite passionate about is structural biology.
It's that part of science that tries to solve proteins three-dimensionally
for us to study the chemical interaction
among small molecules and different amino acids in the molecule
so that we can make chemical molecules more powerful in medication.
Down-left you can see
the different departments I work with, with thousands of people involved
from the gene editing that I talked about CRISPR/Cas9
to identification campaigns of different chemical molecules
trying to find association constants, biophysical aspects
and the use of AI and machine learning
to pay back all this data together and process different chemical procedures.
Here I highlighted several factors that are known
to be crucial for a drug to reach the clinic and be marketed, and to have an effect on patients.
There are 5 main factors: firstly, identifying the appropriate molecular target.
For this, it is essential to find a causal relationship
supported by scientific and experimental data between the target and the specific disease.
It is necessary to have previous results of what the efficacy may be in the patient.
Next: knowing that we are working for the right tissue.
Proteomics and clinical data are fundamental
to know what the dependence of different tissues on different genes in the human organism is.
Safety is also quite important.
Usually, we carry out a study before starting any project
to find out what the adverse effects or possible pharmacological interactions may be
considering the signaling pathways that inhibiting this protein may have in the organism.
And finally, knowing that the population segment we are focusing on for is the right one.
And obviously, during the development
of a drug, billions of dollars and many, many years of development are required.
From an industrial or private point of view, it is necessary
to know the profit the development of this pharmacological therapy we're getting.
I wanted to make an analogy that I think is crucial in terms of biosanitary research
and the balance between pure research and the clinic.
On the left you can see Astrazeneca's R&D headquarters
and on the right, the health campus, through which we can have molecular diagnostics
patient tissues, as Anais has mentioned, immunotherapy studies such as CAR-T therapies, and so on.
I think that collaboration in research and clinical research
and having these campuses, these foci of knowledge
is fundamental to innovate in science and promote new therapies in the clinic.
And this is something that the University of Murcia should be proud of
such as the IMIB, where I was also at the end of my degree
all the work that is being done in the Arrixaca and now also the inauguration of the health campus.
I want to highlight the importance of new therapies when discovering new drugs
such as molecular diagnostics, genomics, AI, etc.
All these are super innovative techniques that I sometimes do not understand
but they are crucial for the development and discovery of new therapies.
Thanks to the Committee,
the Vice-Dean of Research and Juana Mar'ia Ortiz for having me. It's a pleasure to be here
I am happy to help in any way I can, both to you,
to the Committee and to the students of the University. Thank you very much.
We are very proud of your work and everything you have achieved.
Our passion is teaching and training, so seeing all of you succeed is a great feeling.
You set an example for young people.
You all are brave,curious, intrepid,
willing to move, and you are not afraid of leaving your comfort zone.
Life in Spain is really good. I'm sure you miss a lot of thing there in the UK.
So, what things are stimulating when you work abroad?
Leaving everything you no longer have, like friends, family, behind
What motivates you and keeps you going?
The most important thing get these opportunities
is to try to get out of your comfort zone and be ambitious.
Now I look back and wished I had paid more attention in class.
But in the end being ambitious, being curious
and having that self-motivation is what makes you find opportunities.
I have only been in the UK, I have been here for four years since I left the University of Murcia
and I believe that, as my colleagues have said, English is the global language of science.
In this sense, the UK can offer you many opportunities in terms of research, contacts, and money.
UK is one of the strongest powers at academic level.
I think that in Spain is really ambitious when it comes to research
but I think that collaborating and externalizing our knowledge is necessary to enrich us.
Thanks! Any questions?
Well, we are going to introduce last speaker so that we can have a small discussion
of you of what you think is necessary
to promote research and the challenges that today's society poses. Thank you, Miguel.
Thank you.
Hi!
I don't hear you.
Yes, I was muted.
Thank you for coming.
Manuel is a physiotherapist working at the University of Malaga
Last time we talked you were traveling, I don't know if you're back.
I was in Hungary, but now I'm back.
Well, the floor is yours.
Thanks to the Faculty of Medicine and the Department
of Physiotherapy for having me. It is a pleasure to be here among other young researchers.
I would like to talk about my main field of research
which is motion capture and new technologies in physiotherapy.
I've organized the presentation chronologically
from when I started with the master's thesis until now.
How I have always kept in mind the main idea of movement.
Movement is crucial in physiotherapy and analyzing it is fundamental
Since movement and function are present on daily basis.
So I'm going to make a review of my short career.
I've always focused on what is important in movement and the capture of it, the kinematics.
When we talk about kinematics we talk about the movement of something in space
the movement of articulations and the human being.
Kinematic variables are based on motion and
all the variables that go indirectly from that motion, whether it is velocity or acceleration.
In my master's thesis I focused more on the analysis of movement inside the human body
It is important to analyze inside and outside the human body because there are
structures that are more difficult to track because of the way they unfold within our body.
We developed a series of techniques through ultrasound to track.
We used ultrasound and sensors from outside so tracking would be as reliable as possible.
We did this in the scapula, in vertebrae, etc.
All this to know how this structure moves.
We did in vivo, since it's the most normal situation in which this structure develops.
I focused my thesis on the analysis of movement in general.
What kind of techniques are there to measure and to analyze movement?
All this is linked to more commercial fields like entertainment, motion for movies, video games, and so on.
The four main tools most used for that motion analysis are in this slide.
In my thesis I focused on depth cameras. The ones on the top left.
You have maybe used them on the Wii, and they capture the human body very easily.
They are easy to carry and very cheap.
When I started my PhD, we saw a lot of utility in movement analysis for physiotherapy.
There are some alternatives such as optoelectronic cameras, or vicon systems.
A lot of cameras correlated
obtaining information from the human body, but they require more processing, they are very expensive
and it is difficult to use them in the clinic.
Other options are inertial sensors, like simus and electromagnetic sensors.
Both are placed on the subject, and obtain kinematic data from a specific part
but they can't offer the global analysis of the human body that cameras give us.
Besides, placing something on the person is more complicated. We lose a lot of time, the patient may be uncomfortable with contact, etc.
So depth cameras were very useful.
Depth cameras take an image and depending
on the depth at which it is, it will scan the shape of the human body.
As you see in image B, the objects
that are closer are going to look clearer than those that are further away.
That difference in depth is obtained through a series
of codes and algorithms. With that, the camera can recreate a human body.
On the right, you see how a depth camera takes a body structure
assigns a series of joints to it
and we will obtain kinematic information, depending on how these joints unfold.
In my thesis we validated the use
of the camera in patients with low back pain, or with arthritis.
And how kinematics can help to classify patients according to their severity.
This had been studied before with inertial sensors and optoelectronic systems
but this camera is easy to use, cheap and anyone
in any office or clinic can plug in the camera and obtain kinematic data very easily.
After studying this, I felt that it lacked a little more applicability in the treatment.
It was useful to know how this type of patients and structures move
but it lacked a lot of things. So, I started to get into virtual reality.
This is a different approach when it comes
to working with patients, not only in assessment.
Virtual reality is being used a lot and it's proving to be very useful.
There is a lot of controversy
about terminology, we don't exactly know what can be considered virtual reality.
So, roughly speaking, in the picture you can see how this paradigm is changing.
I am going to talk about total immersive virtual reality, the most popular as of now
and the one we can get more benefit from.
We can create scenarios that cannot be done in a real environment.
In those scenarios
we can create interactions that don't exist in real life or the clinic.
The subject believes that they are inside this virtually created universe
so they evade everything that there is outside.
This has a lot of advantages.
It is also an entertainment tool, this type of technology is used in video games.
With covid, metaverses
and virtual environments are being developed so people can communicate.
If we use all this facility that entertainment gives us, and we take it to the clinic
it can help with adherence or when looking for the motivation sometimes our patients lack.
In addition, we can treat
the three degrees of movements, we have total freedom with this technology.
It can help us to complete any type of therapy or applicability within the treatment.
There are many types of systems, from the easiest to the most expensive.
A first approach is to use the cell phone with cardboards. There are two lenses and you place the cell phone in them.
The problem is that the experience depends on the specifications of the cell phone
the phone runs out of battery
and it heats up very quickly. So it is not the best for research, or the clinic.
There are other goggles that are very expensive, but they are more reliable
they have better screens and better monitoring.
These aren't that good for clinical and day-to-day use.
At the moment, the best for those who want to get into virtual reality and to try out experiences that can be used with patients
are the oculus quest 2 or the meta quest.
They are the cheapest, their quality-price ratio is very good, they are wireless, and they are also used right now for research.
What have we seen using these devices?
They can be used for assessment and treatment.
When it comes to treatment, thanks to the evasion these devices provide
we can do exercises that we wouldn't be able to do otherwise.
Because evasion helps us not
to think about the pathology or whether something hurts or not
such as lumbar colors with a high level of catastrophism, kinesophobia, etc.
Through immersion we can
bring movement to people who find it more difficult in the real world.
Thanks to entertainment
the glasses provide, people are physiologically able to exercise more.
This can be used in populations with low performance, and it is also entertaining.
Some of them are similar
to video games, like games that require movements of the upper limbs
which are being marketed and used in research.
They can also be used in games that can be purchased and that can be part of treatment.
And, hand movements.
The objective here is getting
rid of controllers, which collect this information thanks to sensors inside them.
A lot of work is also being done on capturing the hands, since the glasses have small cameras
that protect the environment and know
where the person is while they are enjoying the experience.
We are studying how we can include our own hands in VR.
which helps us for many hand therapies and other types of treatments.
There are many patients who don't feel comfortable with controllers, and with the hand it's easier to handle these therapies.
This is a really interesting field.
Finally, it is a very good option for assessment.
Controllers and glasses have sensors,
because if we move the glasses the environment also moves.
If we take use all the information
that the game collects from both components
and we extract it and use it to help us in assessment, and to obtain kinematic data
we will have entertained patients in totally controlled environments.
Thank you all!
Here is the website of my group, Clinimetria
in case you are interested in what we do, and my email if you need anything.
Thank you so much!
Thanks for telling us about
challenges, research, health trends and immersive virtual reality for therapy.
We are short of time, so we are not going to have much time to have that brief discussion.
I'm glad that you put your email addresses
so our students can get in touch with you.
So, to sum up
and to get a common answer from all of you
in University, we try to encourage our students to do research from their initial training
so that know about all the possibilities and opportunities they have, and encourage them.
So, how could we improve our curriculum to encourage young people to do research?
For example, in my case
in the last year of Odontology, we had to do our final dissertation
that was our first contact research. And if you were lucky,
you had a tutor who was involved, others wanted to get it out of the way quickly.
And that's when realized research was an option.
In the US, students are involved in research projects from the first year with residents
and they fieldwork. For example, RCPs they need to take data from.
But they understand what research
consists of, they have meetings with research groups, etc.
I think it would be great if there were an elective course or part of another subject dedicated to research from the first year.
I think that not everyone is prepared to be a researcher, it has to be something that you like.
and I also did my final dissertation, then a PhD, and so on.
I also think funding is very important.
Because I started my master's and PhD working and doing research at the same time.
Those years were a bit complicated. Until I got a scholarship a stay, or any other help.
There's that.
One thing that I think is fundamental
is to give students access to internships.
for example in the pharmaceutical
industry in other institutions outside the academic field, or within it.
I think telling the students about all the possibilities is fundamental.
Some people don't even know these options exist
or they have not been offered in an appealing way
that makes students take up more research projects in benefit of their future career.
Maybe research is not for you, but
you can start making decisions about what you want for your future career.
I completely agree with you. Ana'is and Pablo, what do you think?
I agree with you all.
In my case, I spent three months
in London, at Kings College, during my predoctoral stage.
I did not go on a postdoctoral stay, because I was given this opportunity in Madrid.
I couldn't say no, since I
have always wanted to work on cancer and Immunology.
But I have moved around a lot since I started my degree.
I studied biology
at the Autonomous University, but I started my internship in the fourth year.
I think that people who want to start an internship should be encouraged to do so
because the sooner you start, the sooner you get to know the world of research
to create a network of contacts,
and it is also very important to participate in congresses.
During my PhD, I've attended many congresses, both national and international.
And that gives you the chance to meet all kinds of people.
I have not been on a postdoctoral stay
but I did my final dissertation in a laboratory.
an internship at the Molecular Biology Center.
I did my Master's in another laboratory. In the end, you learn things from
all the places you've been that can contribute to your research and open your mind.
I have not gone abroad, but I have tried different things
that have been useful in my day-to-day research and continue to be so today.
I agree with all my colleagues here.
I think we could also implement
in the curriculums that everything we teach has been researched.
Not everything we teach is because
the professors have learned it by infuse science. I think that many students are not aware of that.
I think it is very important to tell them that behind the knowledge we teach at university and biomedical degrees
there was and still is a lot of research.
Teaching in biosanitary degrees, or in biochemistry and biology is based on research.
It would be nice to give them practical
research cases so that they can do research to learn how, for example, a metabolic pathway works.
So, they know that research is behind everything they learn.
I think it is crucial to teach them what the impact of all this knowledge is.
Because you can be learning different techniques, strategies,
and so on, but if you don't know what impact it will have, what good is it?
If you don't understand the bigger picture, that knowledge might get lost.
I think it's important to have curriculum
that shows the impact research can have in the future.
I completely agree.
I believe that some students have already taken that step by being here today
talking in English, teaching and showing their work.
Thanks for giving them advice, examples and tricks
I hope that in a little while they will be the ones
who can set an example for other young people as you are doing right now.
Thank you very much on behalf of the Organizing Committee and the University, it has been a pleasure.
We wish you the best of luck. Thank you very much, see you later.
Intervienen
Anaïs Jiménez Reinoso
Investigadora Postdoctoral. Unidad de Inmunoterapia del Cáncer, Fundación de Investigación 12 de Octubre, Madrid, España.
Investigadora Postdoctoral. Unidad de Inmunoterapia del Cáncer, Fundación de Investigación 12 de Octubre, Madrid, España.
Ignacio Pedrinaci Peñalver.
Investigador Postdoctoral School of dental Medicine, Universidad de Harvard, Cambridge, EEUU.
Investigador Postdoctoral School of dental Medicine, Universidad de Harvard, Cambridge, EEUU.
Mª Concepcion Martinez-esparza Alvargonzalez
Moderadora
Moderadora
Manuel Trinidad Fernández
Dr. en Fisioterapia, Grupo de Investigación Climetría, Universidad de Málaga
Dr. en Fisioterapia, Grupo de Investigación Climetría, Universidad de Málaga
Maria Trinidad Herrero Ezquerro
Miguel Gancedo Rodrigo
Farmacéutico investigador, Astrazeneca, Cambrigde, Reino Unido.
Farmacéutico investigador, Astrazeneca, Cambrigde, Reino Unido.
Pablo Pelegrin Vivancos
Investigador distinguido UM. Subdirector IMIB.
Investigador distinguido UM. Subdirector IMIB.
Propietarios
UMtv (Universidad de Murcia)
Publicadores
Mª Concepcion Martinez-esparza Alvargonzalez
Comentarios
Nuevo comentario
Serie: II Congreso internacional de Investigación Biosanitaria para jóvenes investigadores (+información)
CIBJI 2022. Organizado por la Facultad de Medicina de la UM
Descripción
El Congreso tiene como objetivo ser un punto de encuentro para la investigación biosanitaria y una herramienta de formación complementaria en investigación para los estudiantes de Grado, especialmente de Medicina, Odontología, Farmacia, Fisioterapia y para todos aquellos que realicen investigación biosanitaria.